1
1
1
1
1
2
Why do you think Penny was asked to take her blood pressure several times)
Why do you think Penny was asked to take her blood pressure several times)
Jo explained that the heart and the blood vessels make a closed system of fluid (blood)-filled tubes in the body. As a consequence, the volume of blood, diameter of the vessels, and pressure are directly related. If blood volume increases, or vessel diameter decreases, pressure on the walls of the vessels increases. Likewise, if fluid volume decreases, or vessel diameter increases, pressure in the system decreases.
"Think of it like a water balloon,” said Jo. “If I have a balloon and let out water, the balloon is less stretched, there is less pressure; but if I add more water to the balloon, the pressure on the balloon walls increases.”
“Got it,” said Penny. “So if a person were to decrease their blood volume, say if they had a major cut and were bleeding, their blood pressure would drop?”
“Exactly! Additionally, the length of the vessel and the viscosity, or thickness, of the blood matters. Think about drinking out of a straw; which one is easier to use? One that is of typical length or one that is five feet long? The shorter straw is easier to use because there is less resistance. Likewise, what is easier to suck up through a straw, a thick milkshake or orange juice?”
“Orange juice, for sure!” said Penny. “Sometimes you really have to suck to get a thick milkshake to move in the straw.”
“That’s right. The cardiovascular system works much the same way; longer tubes and thicker blood increase resistance, which means the heart has to generate more force to move the blood, which increases blood pressure.”
"Wow, that’s amazing; I hadn’t realized how important blood pressure is for our health. Are there additional issues I should be aware of because I’m pregnant?”
“Unfortunately, yes,” said Jo. “A woman’s body goes through all sorts of physiological changes during pregnancy. In some cases, pregnant women develop high blood pressure and if that happens there can be risks to both the mother and the baby. I don’t know as much about specifics, though. We should consult Google Scholar and the American College of Obstetrics and Gynecologists webpage for information so that you’re prepared for your appointment in the morning. Sound okay?”
“Yes, that sounds great.”
Jo and Penny grabbed the computer and found helpful peer-reviewed publications that discussed the physiology of pregnancy. Jo was currently enrolled in a Master of Science program, so she had experience with credible scientific articles and helped interpret some of the complicated information for Penny.
They read about the maternal-placental (uteroplacental) and fetal-placental (fetoplacental) blood circulation. The mother and the fetus each have their own blood supply and that blood does not mix (at least typically). The placenta is the organ of gas, nutrient, and waste transfer. The fetus is connected to the placenta via the umbilical cord (houses the umbilical artery and vein) and the placenta is implanted into the mother’s uterus. As pregnancy progresses, the placenta becomes more developed and the mother’s vascular network within the placenta grows; there are new spiral arteries, intervillous spaces (funnel-shaped areas that aid in exchange with fetal blood), and veins. The remodeling of the utero-placental vasculature is typically complete by weeks 20–22 of pregnancy.
They also found typical cardiovascular changes that occur in the mother during pregnancy include:
• A 40–50% increase in plasma volume.
• A 25% increase in red blood cells (RBC), but a decrease in overall hematocrit and hemoglobin concentration.
• A decrease in vascular resistance driven by fetoplacental developmental changes, a decreased sensitivity of the mother to angiotensin, and increased production of nitric oxide and relaxin.
• An increase in arterial compliance.
• A 30–50% increase in cardiac output, driven by an increase in both stroke volume (about a 30% increase) and heart rate (about a 15% increase).
After their web browsing session, Jo and Penny felt that they had looked up enough information for one night and were finally able to fall asleep.
The mother and the fetus each have their own blood supply and that blood does not typically mix.
The fetus is connected to the placenta via the
During pregnancy, the cardiovascular system changes. What is the increase of plasma volume?
The next day Penny went to her doctor’s appointment. When she arrived, a nurse took her vital signs and asked Penny to provide a urine sample for further analysis. Penny complied and was escorted to the exam room.
When Dr. Vasandani entered the room, Penny reported her vomiting, headaches, and nosebleed she experienced the day before. She also mentioned the discussion she had had with Jo about blood pressure, and their conclusion that pregnant women should generally have lower rather than higher blood pressure.
Dr. Vasandani was impressed that Penny had done so much background research and reading. However, he was still very concerned about her symptoms. He looked at her chart to find the blood pressure value that the nurse had taken when she arrived; it was 148/90 mmHg.
Throughout his assessment of Penny, he asked a variety of questions regarding her diet, exercise, familial history, and home medications, all of which are factors that can attribute to hypertension. After considering Penny’s background information, Dr. Vasandani recognized that none of these risk factors for hypertension were applicable to Penny.
“Penny, based on the new symptoms you told me about and today’s blood pressure reading, I’d like to do some more tests to find out what’s going on. High blood pressure can be especially dangerous in pregnancy because it can be associated with a diagnosis of preeclampsia.”
Penny was now really worried. She didn’t understand what preeclampsia was; she couldn’t believe that all of this was happening to her. “Dr. Vasandani, I’m very concerned for my baby’s health, as well as my own. Could you please explain to me what exactly preeclampsia is?”
“Absolutely.” He went over to the white board in his office and explained.
What is preeclampsia?
What are some symptoms of preeclampsia?
What symptoms of preeclampsia does Penny have?
This new information made Penny even more anxious because she had never had high blood pressure before and had always lived a healthy lifestyle. The doctor advised her to stay calm and explained that they were going to run some further tests. First they needed to get at least one more blood pressure reading and a measure of the protein in her urine over a 24-hour period. Penny was instructed to take the provided containers home and, starting the next morning, collect all urine produced in the next 24 hours. She was to note the time of first urination and discard that sample.
She was then to collect all urine for 24 hours and keep it cool, either in the refrigerator or on ice in a cooler and then return the samples. The technicians would look for protein in her urine. Protein in the urine can be a sign of multiple physiological conditions. Elevated blood pressure can cause issues with several physiological systems, one of which is the renal system. Prolonged increase in blood pressure can damage the glomeruli of the nephrons, leading to protein leaking into the filtrate and ultimately into the urine.
Dr. Vasandani said he would provide a laboratory analysis of her urine immediately and call her as soon as the results were available. Penny was also instructed to have Jo take her blood pressure that evening before going to bed, and then again in the morning before getting out of bed. Dr. Vasandani’s office would take it again when she returned
with the urine. Penny nodded in agreement. Dr. Vasandani handed Penny two reference sheets on preeclampsia and a flyer explaining how to properly take one’s blood pressure.
Even though he knew Jo was an EMT, he emphasized the importance of following the proper protocol for collecting a blood pressure reading. Penny hurried home to read her resources and talk with Jo.
List 5 things that Jo should do when taking Penny's blood pressure in order to get an accurate reading with the sphygmomanometer. You may use credible sources such as the American Medical Association or the American Heart Association.
Why do you think Penny was asked to take her blood pressure several times)

Calculate Penny's pulse pressure for
160/110 mmHg.
Calculate the MAP for 160/110 mmHg. You will need to use the pulse pressure you found in #14
Calculate Penny's pulse pressure for
148/90 mmHg.
Calculate the MAP for 148/90 mmHg. You will need to use the pulse pressure you found in #16
Typically, preeclampsia is diagnosed by hypertension and increased proteinuria (elevated protein in the urine). There are other factors that influence preeclampsia, including thrombocytopenia, renal insufficiency, impaired liver function, and systematic erythematosus lupus (SLE). However, Penny met criteria for both of the traditional markers and thus likely had preeclampsia. Dr. Vasandani called Penny back to his office to share the news.
“Penny, based on your diagnostic results, such as the proteinuria and consistent hypertension, I am concluding that you have developed preeclampsia.”
Penny started to cry.
“I know this is scary news,” said Dr. Vasandani. “We’ll take good care of you. I’m going to put you in the hospital on bed rest so that we can keep a close eye on you and help to track and monitor your symptoms. With proper care, babies that are delivered at 29 weeks can grow up to be happy and healthy children. I’d like to see if we can get you to 32 weeks, as odds of complications decrease with every additional week of intrauterine fetal development.”
Penny called Jo to come to the office and explained the situation. Penny was admitted to the hospital. They were both incredibly concerned and continued to do additional research on preeclampsia.
What causes preeclampsia?
What are the risks to the baby if preeclampsia occurs?
What are the risks to the mother if preeclampsia occurs?
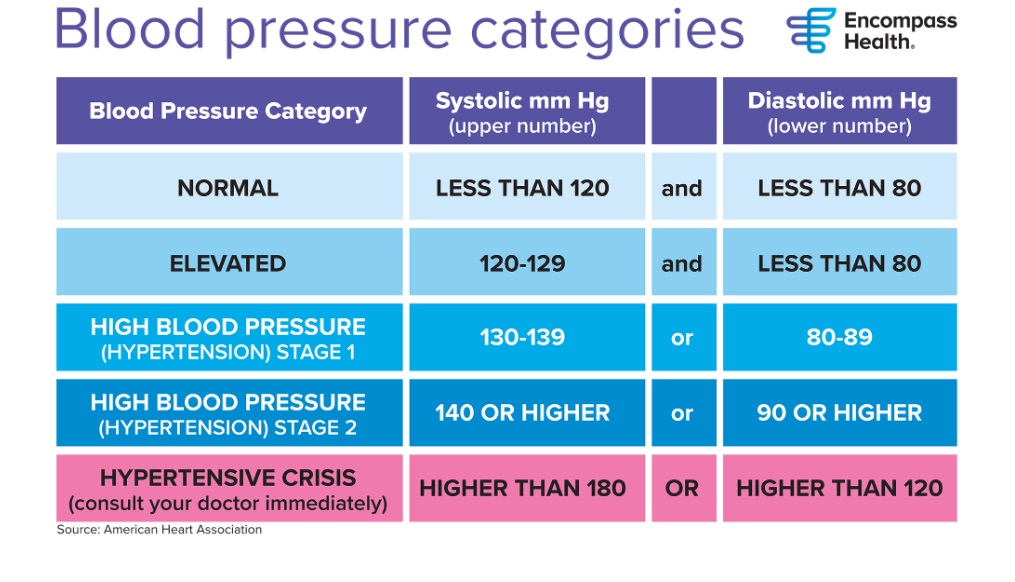
Provide the blood pressure classification for Penny's reading:
Initial Blood Pressure at Home: 160/110 mmHg
Provide the blood pressure classification for Penny's reading:
Blood pressure in office (initial reading): 148/90 mmHg
Provide the blood pressure classification for Penny's reading:
Blood pressure before bed (142/89 mmHg)
Provide the blood pressure classification for Penny's reading:
Blood pressure upon waking at home (135/89 mmHg)
Provide the blood pressure classification for Penny's reading:
Blood pressure in office (160/95 mmHg)
Normal MAP is around 95 mmHg. Is Penny's MAP in the normal range?